Performing a perfect targeted axillary dissection with Magseed® at the Royal Marsden
During a recent training webinar, Mr Peter Barry of the Royal Marsden Hospital in London, explained how they are successfully using Magseed® for lymph node marking.
The webinar was part of the ongoing ATNEC trial study, which aims to evaluate axillary treatment post-neoadjuvant chemotherapy (NAC) in early stage breast cancer patients with no residual disease on sentinel lymph node biopsy.
→ Find out how to take part in the ATNEC study
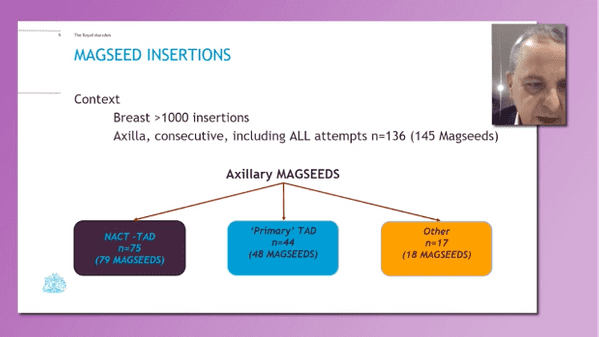
Specialists with experience in node marking were invited to speak, including consultant breast surgeon Mr Barry, who’s centre have now completed over 1,000 Magseed® placements, with almost 150 of these in the axilla.
During the presentation, Mr Barry explained how there are many potential benefits of using Magseed® for node marking. From the patient perspective, it uncouples placement from the day of surgery, and it avoids radioactive solutions and the uncomfortable guidewire.
He told how it’s much easier for physicians too. Royal Marsden radiologists have reported it to be simple to insert and have reported improvements in their workflow, while surgeons find transcutaneous detection straightforward and like that it can be paired with Magtrace® for node marking.
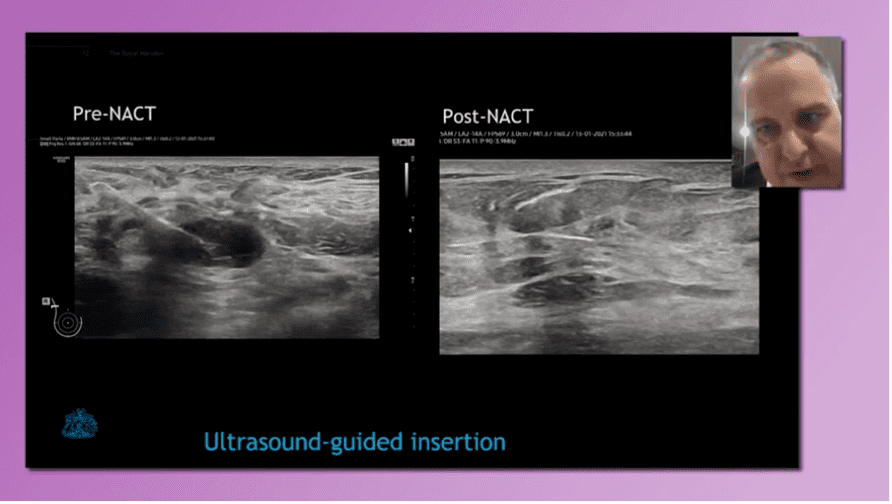
Mr Barry explained that they perform the procedure under ultrasound guidance, as Magseed® is always clearly seen on imaging.
Following this, he explained the evolution of TAD with Magseed® at the Royal Marsden – driven by the wealth of clinical data already available – and the results that they have seen.
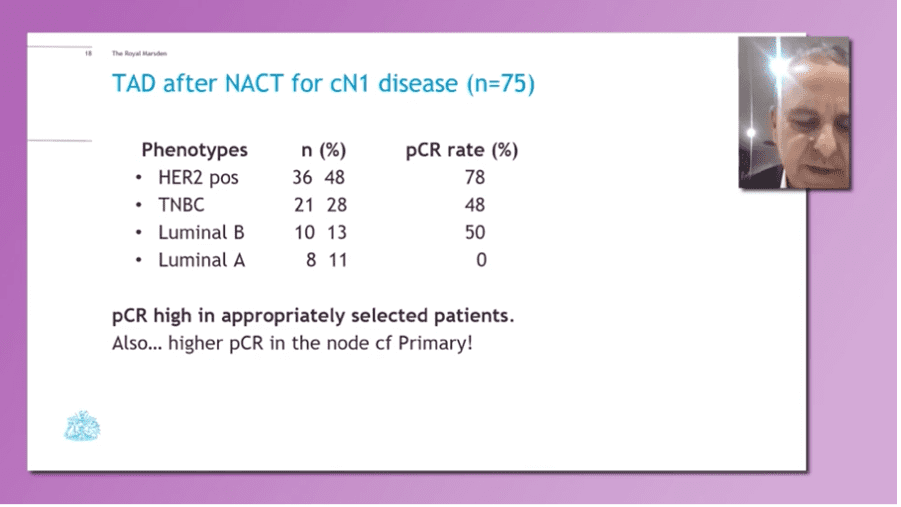
From patients undergoing TAD after NACT for cN1 disease, results varied dependent on the cell subtypes. For example, 78% of HER2 positive patients experienced a pathologic complete response (pCR) with chemotherapy, in comparison to 48% of Triple Negative patients and 0% in Luminal A.
This has encouraged the Royal Marsden to become more selective with the patients put forward for targeted axillary dissection, selecting the subtypes where it can make more of a difference.
At the close of the presentation, attendees were shown a TAD procedure with two Magseed® placements, demonstrating the simplicity of sensing the marked nodes, removing them and confirming that the right nodes have been retrieved.
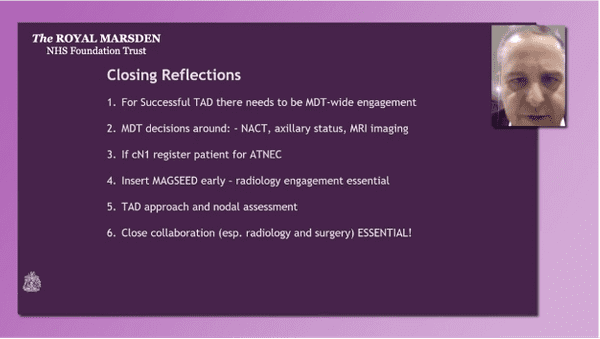
In his closing remarks, Mr Barry explained that there are some key tips that must be followed for successful targeted axillary dissection to take place:
After the presentation, viewers were invited to ask questions – with the first centred on available training resources for using Magseed®. Mr Barry explained that Endomag video resources are available online and the Royal Marsden will soon be uploading their own too.
The session moderator, Mr Amit Goyal, then explained how the Magseed® marker has been made available free to all centres using it on a patient involved in the trial.
To conclude, Mr Barry tackled a question on MRI with Magseed® by suggesting that the Royal Marsden had found the procedure more effective by using ultrasound. However, he also shared tips for those wanting to use MRI with Magseed®:
“Have a look at the original MRI… if the distance between the node and primary is 4cm or closer, use a temporary marker then place the Magseed® in at the end [of the course of NAC]”Mr Peter Barry Royal Marsden Hospital, London